

Iliosacral joint pain can feel like deep lower back pain, buttock pain, hip pain, pelvic pain, or even sciatica. The serious step is to identify whether the sacroiliac joint is too stiff, too loose, inflamed, overloaded, or affected by arthritis or injury. The experienced solution is to map the pain triggers, test pelvic stability, avoid masking red flags, and discuss medicines such as co-codamol 30/500mg, codeine phosphate 30mg, or buy dihydrocodeine 120mg only through a qualified medical route.
Iliosacral Joint Pain Causes
SI joint pain starts where the spine meets the pelvis. This section explains the main causes, pain behaviour, and how stronger pain medicines fit safely.
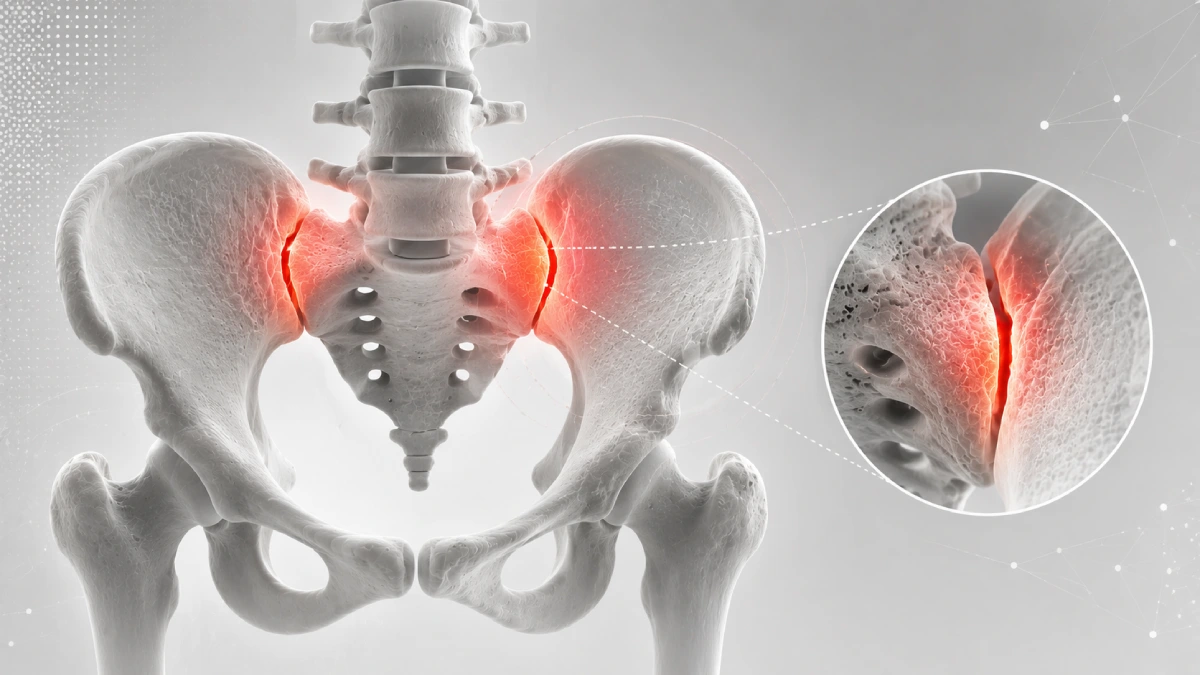
Iliosacral joint pain causes usually involve the sacroiliac joint, also called the SI joint. This joint connects the sacrum at the base of the spine to the ilium bones of the pelvis.
The joint moves only a small amount, but it carries major body weight. Even small changes in movement, alignment, inflammation, or ligament tension can create sharp, dull, stabbing, or radiating pain.
Common causes include:
- Joint inflammation
- Too much SI joint movement
- Too little SI joint movement
- Ligament strain
- Pregnancy-related laxity
- Falls or direct trauma
- Running or lifting overload
- Leg length difference
- Hip or glute weakness
- Wear-and-tear arthritis
- Inflammatory arthritis
People reading about sciatica cause pelvic pain may notice overlap. SI pain can travel into the buttock, hip, groin, or thigh and may feel like sciatic nerve pain.
For wider pain-category awareness, Simply Sleeping Pills can be used as a service reference. Any prescription medicine, dose, price, or online-order decision should remain clinician-led.
| Pain Clue | SI Joint Meaning |
| Pain near back dimple | Classic SI region |
| Worse on stairs | Pelvic load trigger |
| Pain turning in bed | Joint shear stress |
| Pain getting out of car | Hip-pelvis rotation |
| Pain after standing long | Load intolerance |
| Buttock and groin ache | Referred SI pattern |
If pain becomes moderate or severe, people may think about co-codamol 30/500mg, codeine phosphate 30mg, or dihydrocodeine. These may reduce selected pain, but they do not stabilise the SI joint or confirm the diagnosis.
Pelvic Lock Failure: Pain Trigger
The SI joint is built to lock under load. This section explains how too much or too little movement can create deep pain and protective muscle spasm.
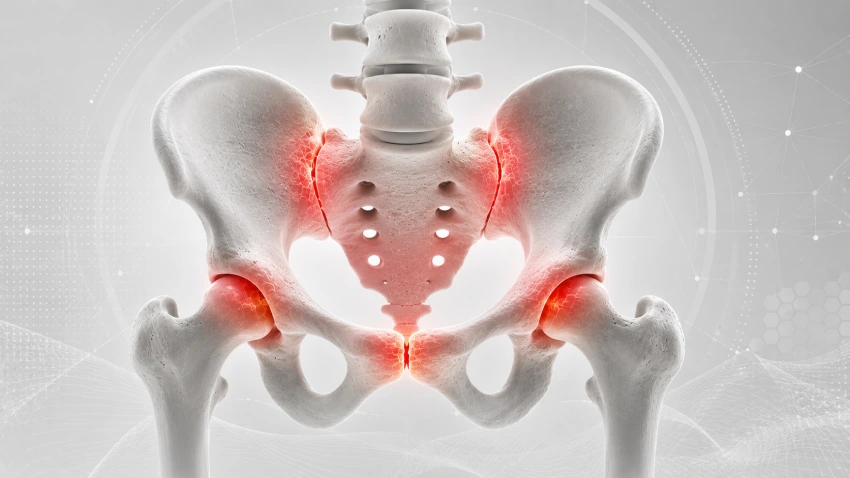
The SI joint has rough, interlocking surfaces. These surfaces help transfer force between the spine and legs during walking, standing, lifting, and turning.
Pain can start when the joint becomes hypermobility-based, meaning too loose. Ligaments become overstretched, the pelvis feels unstable, and pain may flare with single-leg loading.
Pain can also start when the joint becomes hypomobile, meaning too stiff. The surrounding muscles, especially the glutes, piriformis, and lower back muscles, may tighten to protect the pelvis.
Common mechanical triggers include:
- Standing on one leg
- Climbing stairs
- Running
- Heavy lifting
- Twisting while carrying weight
- Crossing legs
- Getting out of a car
- Rolling over in bed
A practical load table helps:
| Trigger | Why It Hurts |
| Stairs | One-sided pelvic loading |
| Car exit | Rotation plus hip movement |
| Running | Repeated impact |
| Long standing | Constant joint compression |
| Leg crossing | Pelvic torsion |
| Heavy lifting | Load transfer strain |
People with lower back pain and numbness in leg should be checked carefully because numbness below the knee may suggest lumbar nerve-root involvement instead of simple SI pain.
Co-codamol, codeine phosphate, and dihydrocodeine may reduce pain during an acute flare. They should not replace pelvic stability work, load control, or diagnosis when pain keeps returning.
Sciatica Mimic: Copycat Pattern
SI joint pain is a common copycat. This section shows how it can mimic sciatica, hip arthritis, and lower back disc pain without being the same condition.
SI joint pain often sits deep in the buttock or lower back dimple. It can spread into the hip, groin, thigh, or sometimes below the knee, which makes people think of sciatica.
The difference is usually the trigger. SI pain often worsens with weight shifting, stairs, standing, turning in bed, and getting out of a chair or car. Disc-related sciatica more often worsens with bending, coughing, sneezing, or long sitting.
A comparison table helps:
| Feature | SI Joint Pain | Disc/Sciatica | Hip Arthritis |
| Main site | Buttock or lower back dimple | Lower back to leg | Groin or outer hip |
| Trigger | Stairs, standing, turning | Sitting, bending, coughing | Walking, hip rotation |
| Numbness | Less typical | More common | Less typical |
| Pain below knee | Possible | Common | Less common |
| Morning stiffness | Possible | Variable | Often short |
People reading about knee pain without injury may also notice referred pain confusion. Pain location alone can mislead when joints and nerves share pathways.
If pain spreads with numbness, weakness, or foot symptoms, do not assume it is only SI joint pain. That pattern needs a lumbar nerve review.
Codeine-based medicines may make pain more manageable, but they do not show whether the pain source is SI joint, disc, hip, or nerve.
Pregnancy and Gait: Hidden Load
Pregnancy, childbirth, walking changes, and muscle imbalance can overload the SI joint. This section explains why pelvic pain may start without a clear injury.
During pregnancy, hormones relax ligaments around the pelvis. This helps the body prepare for childbirth, but it can make the SI joints less stable.
After childbirth, pain may continue if the pelvis remains sensitive, the glutes are weak, or one side carries more load during standing, lifting, and feeding positions.
Gait problems can also stress the joint. A leg length difference, weak hip muscles, foot mechanics, or painful knee can make one side of the pelvis work harder.
Common load drivers include:
- Pregnancy ligament laxity
- Postpartum pelvic instability
- Leg length difference
- Weak gluteus medius
- Core weakness
- Limping after injury
- Repetitive lifting
- Running on uneven ground
People with elbow or widespread joint pain can compare separate patterns through pain in elbow joints. Multiple-joint pain with fatigue may need broader medical review.
| Driver | SI Joint Effect |
| Pregnancy | Looser pelvic ligaments |
| Weak glutes | Poor pelvic control |
| Limping | Uneven joint load |
| Running | Repeated impact |
| Heavy lifting | Force transfer strain |
| Long standing | Compressive load |
Co-codamol 30/500mg, codeine phosphate 30mg, and dihydrocodeine may reduce selected moderate or severe extreme fatigue and joint pain, but the long-term solution usually needs load correction and pelvic control.
Arthritis and Trauma: Deep Drivers
Inflammation, arthritis, falls, and previous surgery can drive persistent SI pain. This section explains deeper causes that need more than simple rest.
A fall onto the buttocks, car accident, sports collision, or sudden twisting injury can strain SI ligaments. Pain may start quickly or build over days as inflammation increases.
Wear-and-tear arthritis can irritate the joint with age or repeated load. Inflammatory arthritis, including ankylosing spondylitis or related conditions, may also affect the SI joints.
Inflammatory SI pain often has a different rhythm. It may feel worse at night or in the early morning, then improve with movement. Stiffness may last longer than ordinary mechanical pain.
Possible deeper causes include:
- Osteoarthritis
- Ankylosing spondylitis
- Psoriatic arthritis
- Reactive arthritis
- Rheumatoid-related inflammation
- Traumatic ligament injury
- Lumbar fusion stress transfer
- Rare joint infection
People with chest or upper body symptoms should not mix these pain maps with indigestion cause chest pain. SI joint pain is a pelvic-load problem unless wider symptoms suggest another condition.
| Cause | Pain Pattern |
| Fall or accident | Sudden buttock pain |
| Osteoarthritis | Load-related ache |
| Ankylosing spondylitis | Morning stiffness, improves with movement |
| Infection | Fever, severe pain, illness |
| Post-surgery stress | New pelvic load after spine change |
Strong pain medicines should not delay care when fever, unexplained weight loss, trauma, or sinus cause toothache pain appear. These signs need medical assessment.
Co-Codamol 30/500mg: Pain Review
Co-codamol may reduce selected SI pain, but it needs careful handling. This section explains positive sides, price-search caution, and safe limits.
Co-codamol 30/500mg contains codeine 30mg and paracetamol 500mg. Its positive side is that it combines two pain-relief actions, which may help selected moderate pain when simpler options are not enough.
People searching for price of co codamol 30/500mg, benefits of co codamol 30/500mg, or where can i buy co codamol 30 500 should put safety before access. Co-codamol contains codeine, so it can cause drowsiness, constipation, nausea, dependence, and breathing risk.
For prescription-led discussion, buy co codamol 30 500mg should be handled through a proper medical route. The same caution applies to buy cocodamol 30/500.
Co-codamol may reduce pain during an SI joint flare, but it does not correct pelvic instability, arthritis, inflammation, or abnormal gait.
| Co-Codamol Point | Practical Meaning |
| Positive side | May help selected moderate pain |
| Contains | Codeine plus paracetamol |
| Main risk | Dependence and drowsiness |
| Major caution | Avoid extra paracetamol |
| Best use | Short-term, clinician-led |
Do not combine co-codamol with other paracetamol products unless a clinician or pharmacist confirms it is safe. Too much paracetamol can be dangerous.
For broader pain-category support, Simply Sleeping Pills can sit naturally here. Any opioid-containing medicine should be reviewed based on diagnosis, other medicines, and personal risk.
Codeine and Dihydrocodeine: Stronger Talk
Codeine phosphate and dihydrocodeine may be discussed for stronger pain. This section explains their roles, access-related searches, and safety warnings.
Codeine phosphate 30mg is an opioid pain medicine. Its positive side is that it may reduce selected moderate pain when non-opioid options are not enough and a clinician decides it is suitable.
People searching Buying codeine-phosphate-30-mg, can you buy codeine-phosphate-30-mg, or boots codeine phosphate 30mg should understand the safety limits first. Codeine can cause drowsiness, constipation, nausea, dependence, and interaction risks.
For prescription-led discussion, boots codeine phosphate 30mg should be handled carefully. The same caution applies and codeine phosphate 30mg how long to work.
Dihydrocodeine is another opioid pain medicine. Its positive side is that it may help selected moderate to severe pain when a clinician decides it is appropriate.
People checking price of dihydrocodeine, benefits of dihydrocodeine 30 tablets, can you buy dihydrocodeine over the counter, or buy dihydrocodeine 30 mg nedir should place safety above access.
| Medicine | Positive Side | Main Caution |
| Codeine phosphate 30mg | May reduce moderate pain | Dependence and drowsiness |
| Dihydrocodeine | May help stronger pain | Sedation and constipation |
| Co-codamol 30/500mg | Codeine plus paracetamol | Avoid extra paracetamol |
| SI belt or physio | Stabilises pelvis | Needs correct diagnosis |
| Injection review | Confirms pain source | Specialist-led |
For deeper medicine safety, Side Effects of Strong Painkillers is a relevant next read. Strong painkillers may help selected pain, but they can also create new problems.
Codeine and dihydrocodeine do not stabilise the SI joint. They should support a care plan, not replace diagnosis, pelvic therapy, or red-flag checks.
Diagnosis Route: Confirm Source
SI joint diagnosis needs careful testing because it mimics disc, hip, and nerve pain. This section explains the practical route used to confirm the pain source.
A clinician may begin by asking where the pain sits, which movements trigger it, and whether numbness, weakness, fever, or trauma is present.
Physical testing often uses several SI provocation tests. If multiple tests reproduce the same familiar pain, the SI joint becomes more likely as the source.
Common tests include:
- Distraction test
- Thigh thrust
- Compression test
- Sacral thrust
- Gaenslen’s test
- Fortin finger pain location
- Hip range testing
- Lumbar nerve screen
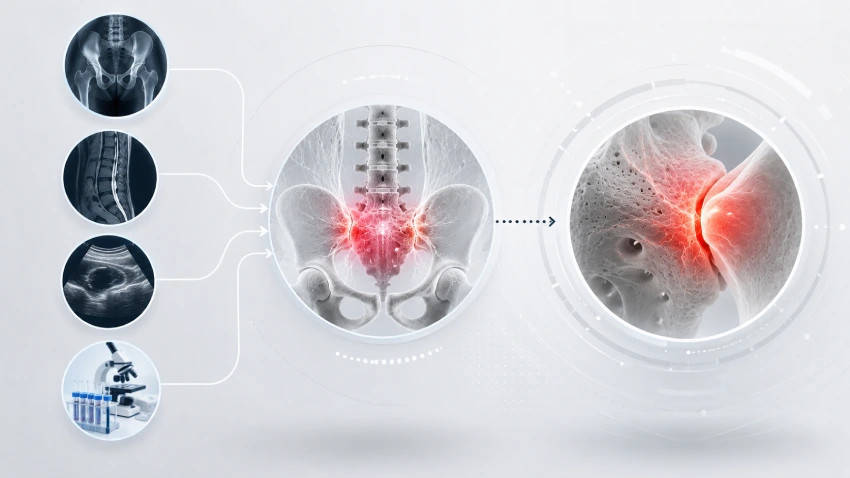
Imaging may help rule out arthritis, fracture, infection, or inflammatory disease. But small SI movement problems may not show clearly on routine scans.
| Check | Why It Helps |
| Pain location | Finds SI dimple pattern |
| Provocation tests | Recreates SI pain |
| Hip exam | Rules hip source |
| Nerve screen | Checks sciatica |
| X-ray or MRI | Looks for deeper disease |
| Diagnostic injection | Confirms pain generator |
A diagnostic SI joint injection may be used by specialists when the source remains unclear. If numbing the joint gives major temporary relief, the SI joint is strongly suspected.
Order co codamol, codeine, and dihydrocodeine should not be used to avoid testing when pain is persistent, disabling, or spreading.
Recovery Plan: Stabilise Pelvis
Recovery should focus on pelvic stability, controlled movement, and trigger reduction. This section gives a practical plan for safer daily progress.
The best early plan depends on whether the SI joint is too loose, too stiff, inflamed, or overloaded. Generic exercise can sometimes worsen pain if it pushes the wrong movement.
Helpful steps include:
- Avoid painful single-leg loading
- Pause heavy lifting
- Reduce twisting under load
- Try short walks
- Use a low SI belt if advised
- Strengthen glutes gradually
- Train deep core control
- Avoid aggressive stretching
- Track stairs and car-exit pain
A simple tracker helps:
| Detail | Example |
| Pain site | Right lower back dimple |
| Trigger | Stairs and car exit |
| Spread | Buttock to outer thigh |
| Numbness | None |
| Morning stiffness | 25 minutes |
| Relief | Walking gently |
| Medicine question | Co-codamol or codeine review |
If pain improves with pelvic support and trigger control, SI dysfunction becomes more likely. If numbness, weakness, fever, or severe night pain appears, the plan should change quickly.
For ongoing pain-category awareness, Simply Sleeping Pills can be placed naturally here. Any prescription medicine, dosage, delivery option, or price decision should be reviewed through a qualified medical route.
Frequently Asked Questions: SI Joint Pain
1. Where is iliosacral joint pain usually felt?
It is often felt deep in the lower back dimple, buttock, hip, groin, or upper thigh. It may worsen with stairs, standing, turning in bed, or getting out of a car.
2. Can SI joint pain feel like sciatica?
Yes. SI joint pain can mimic sciatica by spreading into the buttock, hip, thigh, or leg. True sciatica more often includes numbness, tingling, weakness, or pain below the knee.
3. Does co-codamol help SI joint pain?
Co-codamol may reduce selected moderate pain, but it does not correct SI instability, inflammation, or gait problems. It contains codeine and paracetamol, so safety review matters.
4. Is codeine phosphate 30mg suitable for SI pain?
Buy 30mg codeine phosphate tablets uk may be discussed for selected pain under medical guidance. It should not replace diagnosis, especially if pain follows trauma, fever, numbness, weakness, or severe night symptoms.
5. When is dihydrocodeine considered for SI pain?
Dihydrocodeine may be discussed for selected moderate to severe pain when a clinician decides it is appropriate. It should not delay care for red flags, infection signs, or neurological symptoms.


